
Operating room by Hikaru Iwasaki (PD USGov-Interior)
In 1946 Frederick Prescott found himself on a table, unable to move. He was completely paralyzed. Two minutes prior he was intravenously injected with 30 mg of d-tubocurarine, and now he was in trouble. He could not open his eyes, speak, or even swallow, and no one in the room was aware of his distress. Another minute ticked by, and his breathing became rapid and shallow. Another minute, and he was terrified. He gasped for breath as his airway filled with mucus. Just as he lost consciousness, his colleagues started artificial respiration and manual compression. It took seven minutes for him to start breathing on his own, and another thirty to regain use of his body. Six hours later, he was right as rain, save for tightness in his chest that persisted for several days. (1)
“To be conscious yet paralysed and unable to breathe is a very unpleasant experience.” – Frederick Prescott
How did Prescott find himself in this situation? Voluntarily, for science of course. Dr. Frederick Prescott was the Research Director at the Wellcome Research Institute, and before his merry band of anesthesiologists used d-tubocurarine as an anesthetic, they trialed it on themselves first, to obtain information on dosing and administration (1). This was considered standard practice in the day, before regulatory agencies existed to frown upon it.
There was a need for another anesthetic, besides nitrous oxide, cyclopropane, and ether, for abdominal and thoracic surgeries. Not only did surgeons desire a complete muscle relaxant, but one that did not produce shock and vomiting. The advent and use of d-tubocurarine in surgery was a great advancement in medicine, but it was not without fault. Of concern was that it did not block pain. Fortunately, Dr. Prescott tested this first. During his harrowing experience strips of adhesive plaster were ripped from hairy parts of his body, producing “considerable pain,” from which he was unable to cry out. d-Tubocurarine produces anesthesia without analgesia. It induces unconciousness, not relief from pain.
To explain how Prescott came to this point, we need to travel back to the 16th century and talk about a mixture we now call curare. Curare was most likely first encountered in the mid 1500’s during the exploration and exploitation of South America. Alonso Perez de Tolosa, in what is now Venezuela, encountered a peaceful tribe called the Bobures. Despite their friendliness, and no doubt prodded by the Conquistadors, the Bobures:
“fought just with blowguns, into which they put tiny arrows, dipped in a poison. These, even if they caused only a slight wound, deprived the victim of his senses for two or three hours, the time it took the Indians to flee, and afterwards he recovered without further hurt (2).”
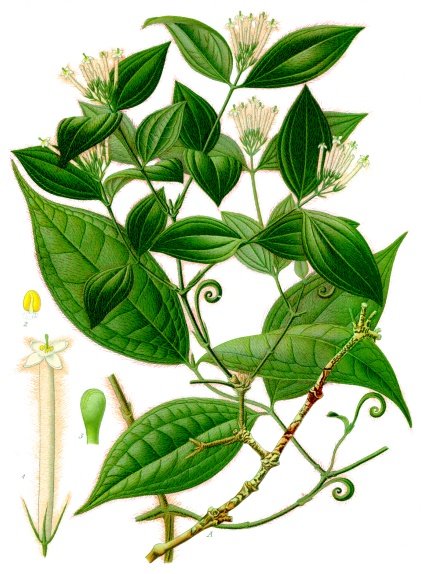
Strychnos toxifera by Koehler (PD-1923)
Curare became almost a catch-all term for any type of arrow poison, and in fact curare was most readily described by what type of vessel it was stored in. We had tube, stored in a bamboo tube, calabash, stored in a gourd, and pot, stored in earthen pots. They not only had a unique use, but a unique preparation. Each was prepared using multiple plant species and other ingredients, and thus contained many different chemicals and alkaloids. The most toxic of the three, tube curare, was typically prepared from the bark of the viney, jungle plant Strychnos toxifera (3). If the genus Strychnos sounds familiar to you, it’s because it happens to be the same genus that includes Strychnos nux-vomica and the poison strychnine (click to read about strychnine’s history and science, or about it in your beer). Native South Americans use curare for hunting wild game. And just like with de Tolosa’s men, wild animals become paralyzed. The prey either die of asphyxiation due to respiratory paralysis or become paralyzed enough for them to be tracked down. Are they afraid of eating poisoned meat? No. Curare has zero, or close to it, oral bioavailability. So unless you make curare BBQ sauce, you’re safe.
Curare is no doubt a useful tool, but with so many components, which one is responsible for the paralytic effects? The answer would have to wait 400 years. It wasn’t until 1935 that Harold King obtained a supply of tube curare from the Museum Department of the Pharmaceutical Society and not only isolated the active component, d-tubocurarine, but determined its structure (4). Do you think d-tubocurarine got its name from “tube curare”? Probably, but d-tubocurarine is in fact produced by Chondrodendron tomentosum, another viney, South American plant whose only relation to Strychnos toxifera is that they’re both plants. I told you the term curare was a catch-all.
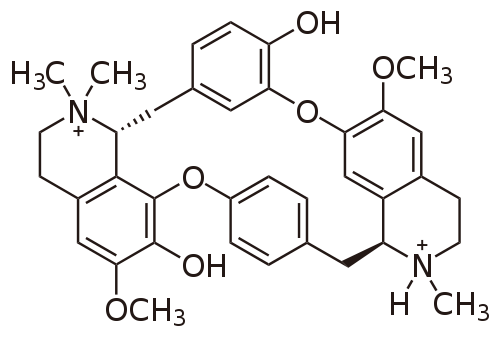
d-Tubocurarine
The mechanism of action is all that is left to explain. d-Tubocurarine is an antagonist of (works against) the nicotinic acetylcholine receptor. The nicotinic acetylcholine receptors form ion-channels, and are activated by acetylcholine and nicotine, just as the name indicates. Their function is to control actions of the peripheral nervous system (PNS), not only by connecting our brain to our extremities, but in neuromuscular junctions, which signal muscles to contract. We know from the nicotine poisoning of King Joffrey that the PNS controls involuntary actions, and we use the mnemonic SLUDGE to remember them: Salivation, Lacrimation, Urination, Defecation, GI upset, and Emesis. This is the autonomic nervous system component of the PNS, which also controls your heartbeat and breathing. But there is also voluntary movement, the somatic nervous system component of the PNS, that occurs via skeletal muscles. Both breathing and moving your arm require muscle contraction and thus neuromuscular junctions. It just so happens that d-tubocurarine works diligently against neuromuscular junctions, and hinders motor functions that we cannot control, like breathing, and ones we can, like moving your limbs. Frederick Prescott learned this first hand. This is why curare, and d-tubocurarine, was so important – as a neuromuscular blocking agent. (For a review, see ref. 5)
Tubocurarine is not as popular as it once was, but its early use led to the development of the second and subsequent generations of neuromuscular blocking agents, namely rocuronium and pancuronium. Curare, and it’s component d-tubocurarine, has made it a long way from an arrow poison first described in the mid-1500’s to a drug still in use today.
POP QUIZ (Answer at the end of the references):
Which one of Nature’s Poisons is an antidote for curare poisoning, and why?
*** [Homepage featured image of blow gun by Yves Picq (CC BY-SA 3.0)] ***
References:
1. Prescott, F. “Tubocurarine Chloride As An Adjunct To Anesthesia.” The Lancet 248.6412 (1946): 80-84.
2. Bisset, Norman G. “War and Hunting Poisons of the New World. Part 1. Notes on the Early History of Curare.” Journal of Ethnopharmacology 36.1 (1992): 1-26.
3. West, Ranyard. “The Pharmacology and Therapeutics of Curare and its Constituents.” Proceedings of the Royal Society of Medicine 28 (1935): 565-578.
4. King, Harold. “Curare Alkaloids. Part I. Tubocurarine.” Journal of the Chemical Society (Resumed) (1935): 1381-89.
5. Bowman, W. C. “Neuromuscular Block.” British Journal of Pharmacology147.S1 (2006): S277-286.
POP QUIZ ANSWER: That would be physostigmine, by way of the Calabar Bean. It works as an acetylcholinesterase inhibitor, thus increasing acetylcholine in the body, and countering curare’s antagonism of nicotinic acetylcholine receptors.

Pingback: Case Study: How Not to Poison Someone | Nature's Poisons
Pingback: That’s a Venomous Snake That Just Bit You, Not a Poisonous One | Nature's Poisons
Pingback: Brugmansia: Angel’s Trumpet or the Devil’s? | Nature's Poisons
Pingback: Toxic Larvae: Arrow Poison from the Bushmen of the Kalahari | Nature's Poisons
Pingback: Green Tobacco Sickness: The Plight of Tobacco Harvesters | Nature's Poisons
Pingback: Guachamacan: A 174-year-old Venezuelan Poison Mystery | Nature's Poisons
Pingback: Self-Experimentation – foamite.org — it's infectious
Justin, saw your site today. Interesting article, but, one error. Paralytics (referred to clinically as muscle relaxants) provide zero anesthesia. They work only on the peripheral nervous system and do NOT cross the blood-brain barrier. Unconsciousness must be induced with some other drug, either inhaled or injected. There are many case reports of patients undergoing surgery who were conscious yet paralyzed and unable to alert the anesthetist they were awake and feeling everything.
Pingback: Antiarin and the Legend of the Upas Tree | Nature's Poisons
1
1
1*1
1′”